Key Results
Key Result 1
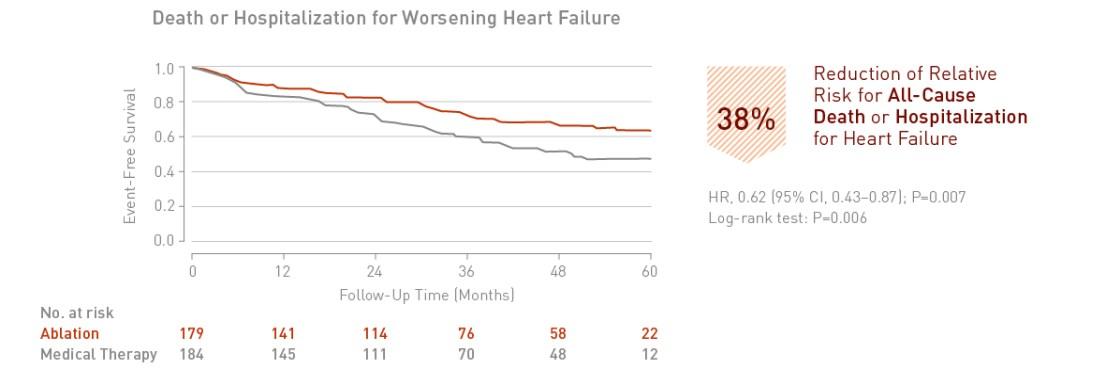
Catheter ablation of atrial fibrillation in patients with heart failure is associated with a significant 38% reduction in death or hospitalization for worsening heart failure.
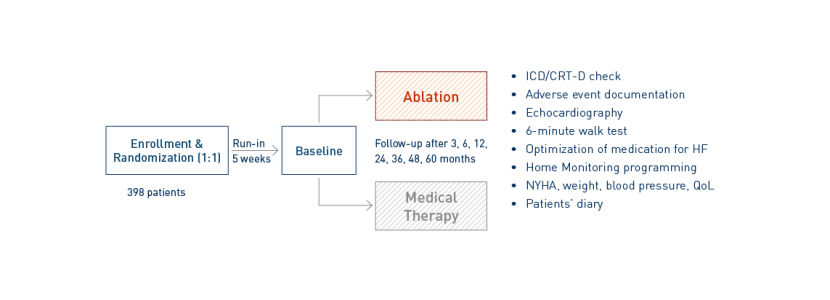
Catheter Ablation Versus Standard Conventional Treatment in Patients with Left Ventricular Dysfunction and Atrial Fibrillation
Marrouche NF, Brachmann J et al., New England Journal of Medicine 2018
Catheter ablation of atrial fibrillation in patients with heart failure is associated with a significant 38% reduction in death or hospitalization for worsening heart failure.
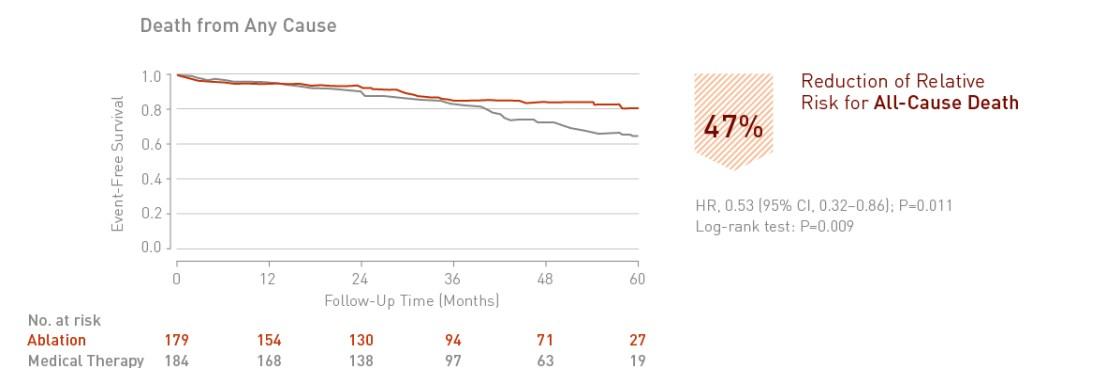
Catheter ablation of atrial fibrillation in patients with heart failure is associated with a significant 47% reduction in death from any cause.
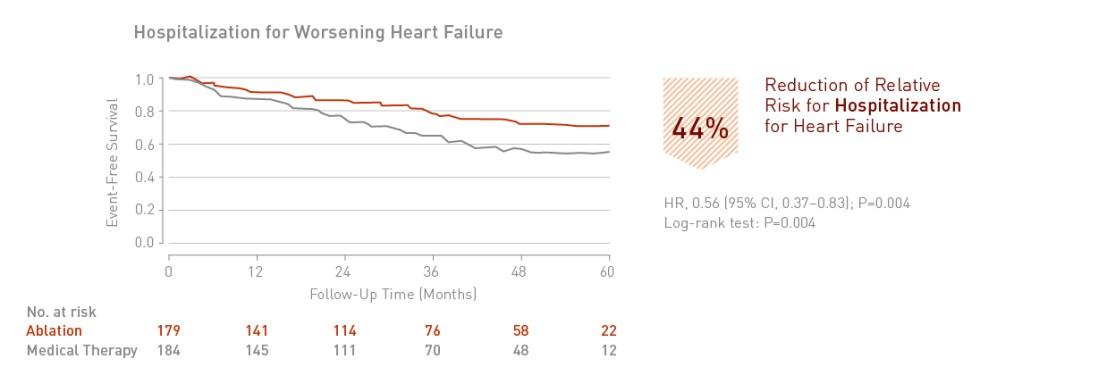
Catheter ablation of atrial fibrillation in patients with heart failure is associated with a significant 44% reduction in hospitalization for worsening heart failure.